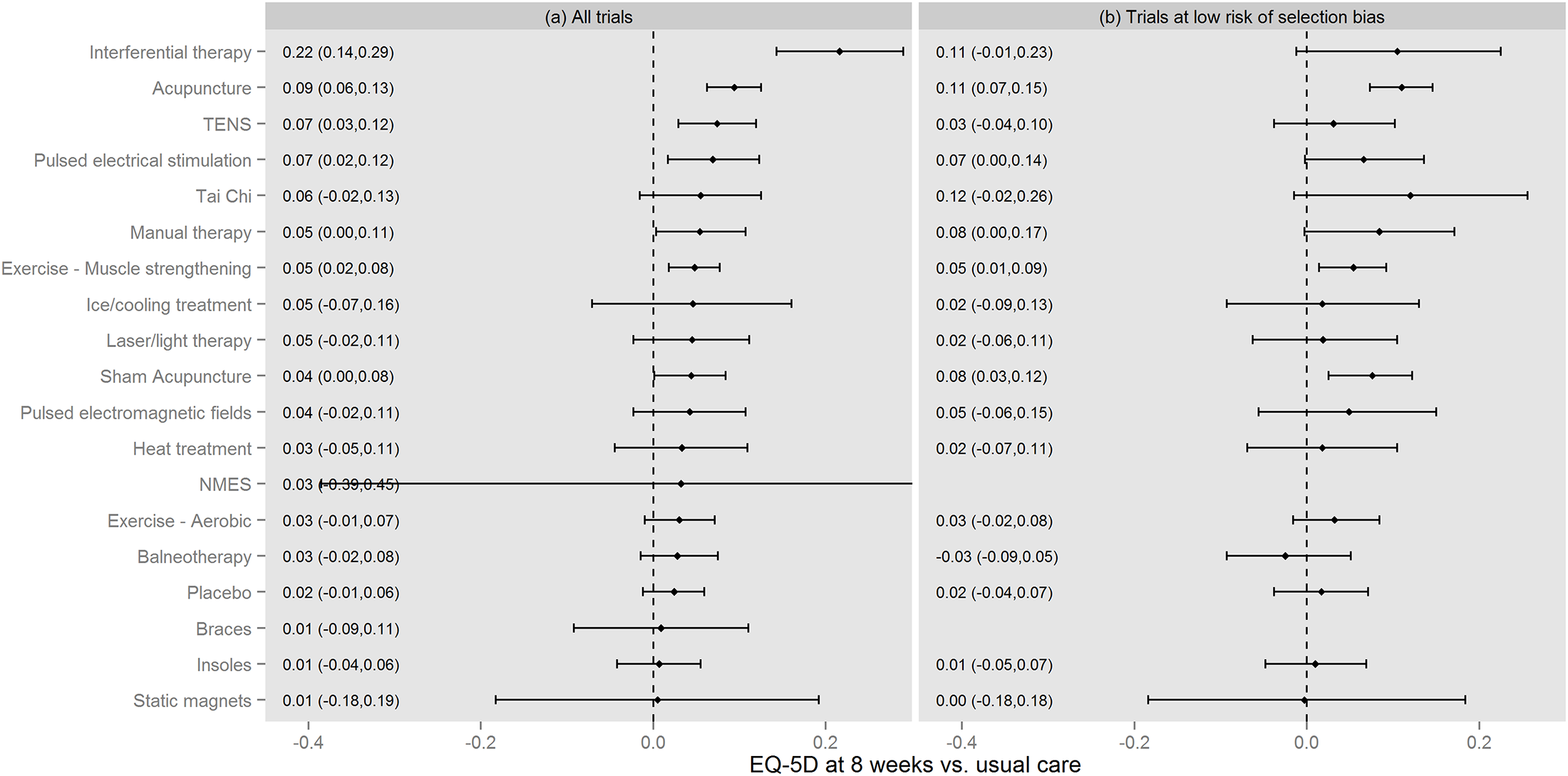
Figure 3 from Woods B et al PLoS One 2017[1]
This figure may seem familiar to some who follow big data in the acupuncture field. It comes from another big project at the Centre for Health Economics, University of York.[1] It is effectively a repeat of their first large network meta-analysis (NMA) that included acupuncture and sham acupuncture in knee osteoarthritis (OA),[2] but this time replacing pain outcomes with health-related quality of life in the form of the EQ-5D aka Euroqol.
There are also overlaps with Saramago et al from 2016,[3] which I wrote about on this blog under the title Quality sham. This paper by Woods et al narrows the view from chronic pain to OA knee alone and extends the analysis to a full cost comparison of non-pharmacological interventions.
This is a thorough piece of work from a well-recognised centre. Whilst data for some interventions was limited, the data for acupuncture and muscle strengthening exercise for example appears fairly reliable; that is, the confidence intervals are tight and the point estimate consistent in both analyses illustrated in the figure above. In total the NMA included 88 RCTs (randomised controlled trials) and 7507 patients.
I suppose the major limitation of this analysis is that there was only data available to calculate outcomes at 8 weeks ie after a course of treatment rather than in the long term. Woods et al cover this aspect in their discussion and put forward an argument for positive commissioning decisions rather than waiting for more evidence.
In terms of EQ-5D outcomes, acupuncture appears to do well, but costs of performing a course of treatment must also be taken into account. When this is done, TENS is the most cost effective intervention, coming in at £2690 per QALY (quality adjusted life year) versus usual care. When only trials with a low risk of selection bias were considered the effect size of TENS dropped and it then came in at £6142 per QALY versus usual care. In this analysis acupuncture then became cost effective at £13 502 versus TENS.
I should note that when all non-pharmacological interventions are considered TENS and acupuncture are the two most cost effective. In the latest clinical guideline from NICE on osteoarthritis (CG177)[4] TENS is recommended, but acupuncture is not.
References
- Woods B, Manca A, Weatherly H, et al. Cost-effectiveness of adjunct non-pharmacological interventions for osteoarthritis of the knee. PLoS One 2017;12:e0172749. doi:10.1371/journal.pone.0172749
- Corbett MS, Rice SJC, Madurasinghe V, et al. Acupuncture and other physical treatments for the relief of pain due to osteoarthritis of the knee: network meta-analysis. Osteoarthritis Cartilage 2013;21:1290–8. doi:10.1016/j.joca.2013.05.007
- Saramago P, Woods B, Weatherly H, et al. Methods for network meta-analysis of continuous outcomes using individual patient data: a case study in acupuncture for chronic pain. BMC Med Res Methodol 2016;16:131. doi:10.1186/s12874-016-0224-1
- NICE guideline update on osteoarthritis: the care and management of osteoarthritis in adults. http://guidance.nice.org.uk/CG177. 2014.
Declaration of interests
I am the salaried medical director of the British Medical Acupuncture Society (BMAS), a membership organisation and charity established to stimulate and promote the use and scientific understanding of acupuncture as part of the practice of medicine for the public benefit.
I am an associate editor for Acupuncture in Medicine.
I have a very modest private income from lecturing outside the UK, royalties from textbooks and a partnership teaching veterinary surgeons in Western veterinary acupuncture. I have no private income from clinical practice in acupuncture. My income is not directly affected by whether or not I recommend the intervention to patients or colleagues, or by whether or not it is recommended in national guidelines.
I have not chaired any NICE guideline development group with undeclared private income directly associated with the interventions under discussion. I have participated in a NICE GDG as an expert advisor discussing acupuncture.
I have used Western medical acupuncture in clinical practice following a chance observation as a medical officer in the Royal Air Force in 1989. My opinions are formed by data that spans the range of quality and reliability, much of which is in the public domain.
I have a logical mistrust of the motives of anyone who advertises an interest or hobby in being a ‘Skeptic’, as opposed to using appropriate scepticism within their primary profession, or indeed organisations that claim to promote generic ‘science’ as opposed to actually engaging in it.