By Dr Nicky Keay

The Endocrine system comprises various glands distributed throughout the body that secrete hormones to circulate in the blood stream. These chemical messengers, have effects on a vast range of tissue types, organs and therefore regulate metabolic and physiological processes occurring in systems throughout the body.
The various hormones produced by the Endocrine system do not work in isolation; they have interactive network effects. The magnitude of influence of a hormone is largely determined by its circulating concentration. This in turn is regulated by feedback loops. For example, too much circulating hormone will have negative feedback effect causing the control-releasing system to down regulate, which will in turn bring the level of the circulating hormone back into range. Ovulation in the menstrual cycle is a rare example of a process induced by positive hormonal feedback.
In the control system of hormone release, there are interactions with other inputs in addition to the circulating concentration of the hormone. The hypothalamus (gland in the brain) is a key gateway in the neuro-endocrine system, coordinating inputs from many sources to regulate output of the pituitary gland, which produces the major stimulating hormones to act on the Endocrine glands throughout the body.
 The Endocrine system displays complex dynamics. There are temporal variations in secretion of hormones both in the long term during an individual’s lifetime and on shorter timescales, as seen in the diurnal variation of some hormones such as cortisol, displaying a circadian rhythm of secretion. The most fascinating and complex control system is found in the hypothalamic-pituitary-ovarian axis. Variation in both frequency and amplitude of gonadotrophin releasing factor (GnRH) secretion from the hypothalamus dictates initiation of menarche and the subsequent distinct pattern of cyclical patterns of the sex steroids, oestrogen and progesterone.
The Endocrine system displays complex dynamics. There are temporal variations in secretion of hormones both in the long term during an individual’s lifetime and on shorter timescales, as seen in the diurnal variation of some hormones such as cortisol, displaying a circadian rhythm of secretion. The most fascinating and complex control system is found in the hypothalamic-pituitary-ovarian axis. Variation in both frequency and amplitude of gonadotrophin releasing factor (GnRH) secretion from the hypothalamus dictates initiation of menarche and the subsequent distinct pattern of cyclical patterns of the sex steroids, oestrogen and progesterone.
So what have the Endocrine system and hormone production got to do with athletes and sport performance?
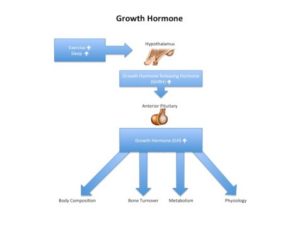
- Exercise training stimulates release of certain hormones that support favourable adaptive changes. For example, exercise is a major stimulus of growth hormone, whose action positively affects body composition in terms of lean mass, bone density and reduction of visceral fat.
- Disruption of hormones secreted from the Endocrine system can impair sport performance and have potential long term adverse health risks for athletes. This picture is seen in the female athlete triad (disordered eating, amenorrhoea and low density) and relative energy deficiency in sport (RED-S) with multi-system effects. In this situation there is a mismatch between dietary energy intake (including diet quality) and energy expenditure through training. The net result is a shift to an energy saving mode in the Endocrine system, which impedes both improvement in sport performance and health. RED-S should certainly be considered among the potential causes of sport underperformance, suboptimal health and recurrent injury, with appropriate medical support being provided.
- Caution! Athletic hypothalamic amenorrhoea, as seen in female athletes (in female athlete triad and RED-S) is a diagnosis of exclusion. Other causes of secondary amenorrhoea (cessation of periods >6 months) should be excluded such as pregnancy, polycystic ovary syndrome (PCOS), prolactinoma, ovarian failure and primary thyroid dysfunction.
- Unfortunately the beneficial effects of some hormones on sport performance are misused in the case of doping with growth hormone, erythropoeitin (EPO) and anabolic steroids. Excess administered exogenous hormones not only disrupt the normal control feedback loops, but have very serious health risks, which are seen in disease states of excess endogenous hormone secretion.
So the Endocrine system and the circulating hormones are key players not only in supporting health, but in determining sport performance in athletes.
References
Sport Performance and RED-S, insights from recent Annual Sport and Exercise Medicine and Innovations in Sport and Exercise Nutrition Conferences British Journal of Sports Medicine 17/3/17
Teaching module on RED-S for British Association of Sport and Exercise Medicine as CPD for Sports Physicians
Optimal Health: Including Female Athletes! Part 1 – Bones British Journal of Sport Medicine 26/3/17
Optimal Health: Including Male Athletes! Part 2 – REDs British Journal of Sport Medicine 4/4/17
Optimal Health: Young athletes! Part 3 Consequences of RED-S British Association Sport and Exercise Medicine 13/4/17
Optimal Health: All Athletes! Part 4 Mechanisms of RED-S British Association Sport and Exercise Medicine 13/4/17
Enhancing sport performance: part 1
Enhancing sports performance: part 3
From population based norms to personalised medicine: Health, Fitness, Sports Performance British Journal of Sport Medicine
Sleep for health and sports performance British Journal of Sport Medicine
Balance of recovery and adaptation for sports performance British Association of Sport and Exercise Medicine
Inflammation: why and how much?
Keay N, Logobardi S, Ehrnborg C, Cittadini A, Rosen T, Healy ML, Dall R, Bassett E, Pentecost C, Powrie J, Boroujerdi M, Jorgensen JOL, Sacca L. Growth hormone (GH) effects on bone and collagen turnover in healthy adults and its potential as a marker of GH abuse in sport: a double blind, placebo controlled study. Journal of Endocrinology and Metabolism. 85 (4) 1505-1512. 2000.
Wallace J, Cuneo R, Keay N, Sonksen P. Responses of markers of bone and collagen turover to exercise, growth hormone (GH) administration and GH withdrawal in trained adult males. Journal of Endocrinology and Metabolism 2000. 85 (1): 124-33.
Keay N. The effects of growth hormone misuse/abuse. Use and abuse of hormonal agents: Sport 1999. Vol 7, no 3, 11-12.
Wallace J, Cuneo R, Baxter R, Orskov H, Keay N, Sonksen P. Responses of the growth hormone (GH) and insulin-like factor axis to exercise,GH administration and GH withdrawal in trained adult males: a potential test for GH abuse in sport. Journal of Endocrinology and Metabolism 1999. 84 (10): 3591-601.
Keay N, Logobardi S, Ehrnborg C, Cittadini A, Rosen T, Healy ML, Dall R, Bassett E, Pentecost C, Powrie J, Boroujerdi M, Jorgensen JOL, Sacca L. Growth hormone (GH) effects on bone and collagen turnover in healthy adults and its potential usefulness as in the detection of GH abuse in sport: a double blind, placebo controlled study. Endocrine Society Conference 1999.
Wallace J, Cuneo R, Keay N. Bone markers and growth hormone abuse in athletes. Growth hormone and IGF Research, vol 8: 4: 348.
Keay N, Fogelman I, Blake G. Effects of dance training on development,endocrine status and bone mineral density in young girls.Current Research in Osteoporosis and bone mineral measurement 103, June 1998.
Keay N, Effects of dance training on development, endocrine status and bone mineral density in young girls, Journal of Endocrinology, November 1997, vol 155, OC15.
Keay N, Fogelman I, Blake G. Bone mineral density in professional female dancers. British Journal of Sports Medicine, vol 31 no2, 143-7, June 1997.
Keay N. Bone mineral density in professional female dancers. IOC World Congress on Sports Sciences. October 1997.
Keay N, Bone Mineral Density in Professional Female Dancers, Journal of Endocrinology, November 1996, volume 151, supplement p5.
Key words: adaptation, amenorrhoea, doping in sport ,Endocrine system, endocrinology, exercise, female athlete triad, fitness, growth hormone, health, hormones, injury, REDs, sport, training