By Daniel Pang
A report of an unexpected and novel anaesthetic complication in a rabbit, the presence of faecal matter in the oropharynx impeding attempts at intubation, was recently published in Veterinary Record Case Reports.
The incidence of anaesthetic- and sedation-related mortality in apparently healthy rabbits is 1.4 per cent, six to eight times greater than in dogs or cats, and respiratory complications represent a substantial fraction of these deaths.
Unfortunately, undiagnosed respiratory disease and hypoventilation due to anaesthetic agents can cause significant respiratory depression. Endotracheal intubation provides a secure airway, facilitating positive pressure ventilation, reducing the risk of fluid aspiration and limits workplace pollution with anaesthetic gases. However, many rabbits are maintained anaesthetised with a face mask, rather than secure airway, because they are challenging to intubate. They have a relatively large tongue, narrow oral cavity and small glottis, which combine to limit visibility of, and access to, the larynyx. Simpler, novel methods of securing an airway such as supraglottic airway devices (eg, Laryngeal Mask Airway, VGel) have shown promise in clinical use.
A healthy, adult New Zealand white rabbit was anaesthetised for a CT scan as part of a larger study evaluating different methods of providing a secure airway to facilitate ventilation. Following induction of general anaesthesia (intramuscular dexmedetomidine and midazolam, followed by intravenous alfaxalone), the rabbit was positioned in sternal recumbency and orotracheal intubation with an endotracheal tube was attempted with a blind technique. Initial attempts at intubation by an experienced anaesthetist were unsuccessful, with intubation finally achieved after five minutes. This contrasted with an average of two minutes to perform intubation in similar rabbits by the same anaesthetist.
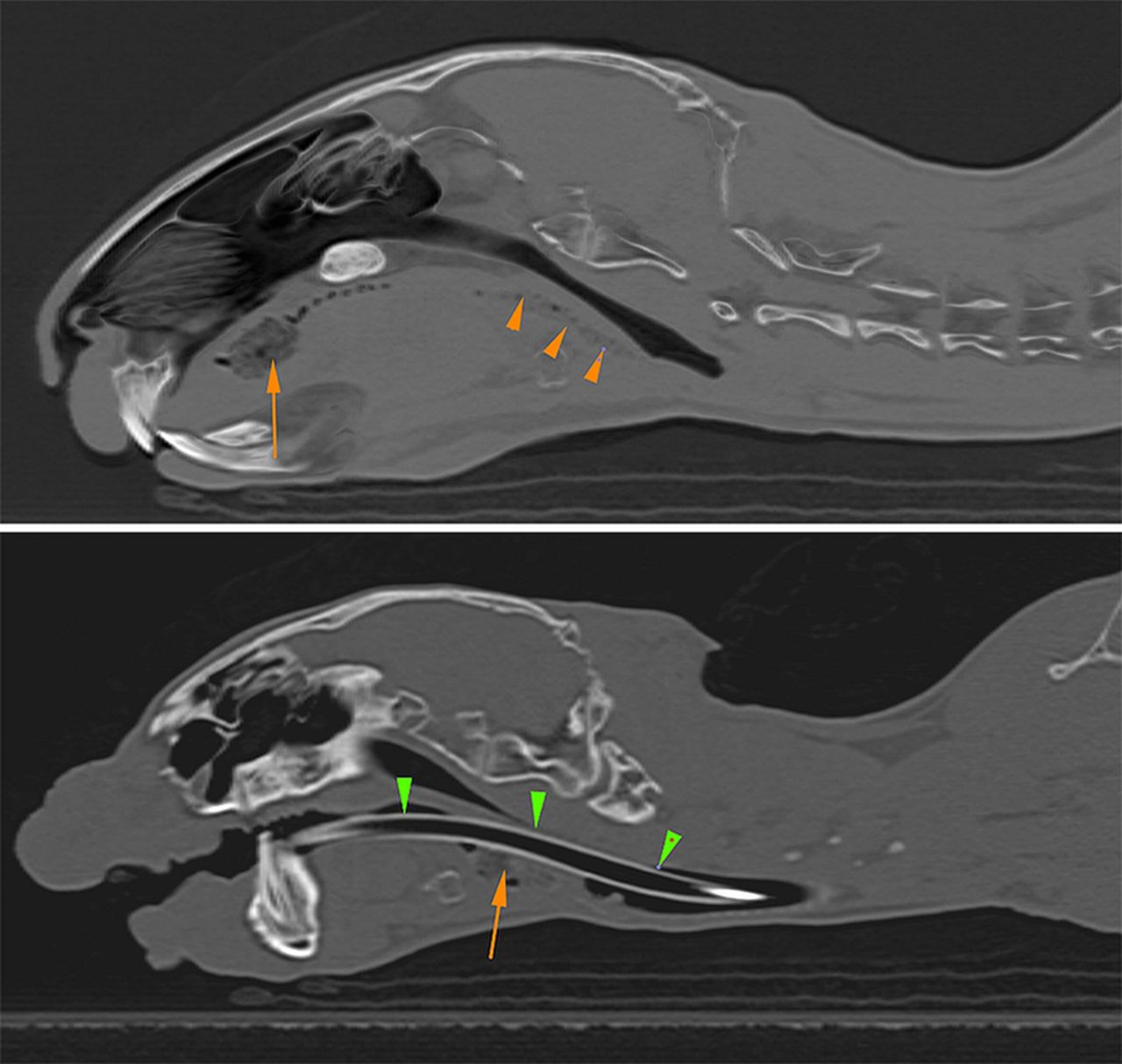
The study protocol required CT scans of the oropharynx to be performed before and after intubation. These ‘pre’ and ‘post’ scans allowed us to identify the cause of the difficult intubation: faecal matter present in the oropharynx before intubation, which was pushed caudally to cause a physical obstruction during attempted intubation (Fig 1). This was also confirmed at postmortem examination.
The source(s) of failed orotracheal intubation attempts in rabbits are usually unknown, although there is a tendency to blame anaesthetist inexperience or anatomical impediments. This report identifies a previously undocumented source of a difficult intubation. A preanaesthetic examination of the oral cavity in rabbits may be warranted, but is unlikely to rule out the presence of foreign material in the oropharynx.
The full article is available here: http://vetrecordcasereports.bmj.com/content/4/1/e000265.full