By Bianca Broadbent @Thecyclingphys
The whole experience of a bike fit is highly complex. It is also an area of ongoing significance for injury prevention. In this blog, I outline the scientific rationale behind bike alignment, and discuss noteworthy trends and how you might utilise these with your current clients.

A proper bicycle fit is essential for comfort, injury prevention, and performance. It optimises power output, aerobic efficiency, aerodynamics, and sustainability for the target event duration (Silberman et al. 2005). Cyclists average between 80-100 pedal revolutions per minute, which equates to around 5400 revolutions per hour. For cyclists riding anything from a few hours per week as a leisure ride, through to competitive cyclists doing 15-20 hours or professional riders doing 30-40 (STOP) hours per week, any ongoing asymmetries or mal-alignments can easily result in injuries and discomfort.
A combination of high training volume and mal-alignment is indicated as an anatomic risk factor for overuse injury (Ahonen 2008, Fousekis et al. 2010, Krivickas 1997). However, quantification of the contribution of asymmetric intrinsic and extrinsic factors to a dose response relationship within musculo-skeletal loading is problematic; norm values do not allude to the epidemiology of asymmetry. The introduction of technology to the bike fitting process through 3D kinematics is starting to produce this database of knowledge.
Use of technology to drive the decision making within bike fitting is a relatively new phenomenon within the cycling world. It has become more popular recently with bike mechanics, coaches, physios, and other health care professionals getting on board. However there is the risk of commercial bias, where companies will use the fitting tools to push their latest products, but do not always identify the most appropriate product for the consumer and their specific injury or complaint.
SO WHAT ACTUALLY IS A BIKE FIT?
Bicycle fitting methods can broadly be categorised into static (measurements taken at rest) and dynamic (measurements taken while riding). Taking from several sources, we may define it as “harmonisation between the rider and the bicycle, based on their goals, injuries and physical capabilities”.
Market leading companies are Specialized, Retül (which now comes under specialized), with alternative approaches include Bikefit.com, Apex, Torke, and Gebiomized which also offer pressure assessment for saddles, feet and handlebars.
Like all tools and techniques it is the operator rather than the software who needs to make the fit decisions. Also, the clinical reasoning skills of an experienced clinician are essential when dealing with a multifactorial presentation.
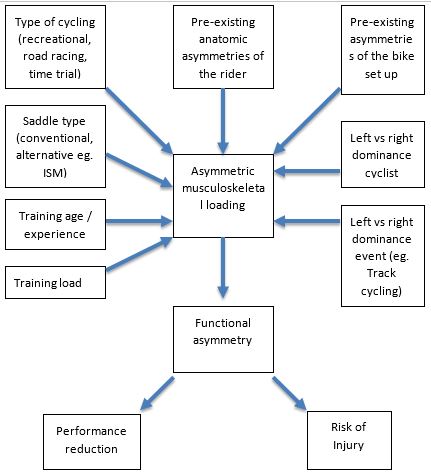
A new theoretical model of factors associated with functional asymmetry in cycling sports
There are three contact points a rider has with the bicycle; shoe-cleat-pedal interface, pelvis-saddle interface, and hands-handlebar interface.
CURRENT TRENDS
The cleats
There are many cleat systems available, Speedplay, Look, Shimano and others, which all offer varying degrees of adjustment, rotation, shimming and wedging. Certainly research seems to suggest allowing cleat float can reduce the incidence of knee pain (Gregor and Wheeler 1994).
There are also many studies linking a poor cleat set up with iliotibial band syndrome (Farrell, Reisinger and Tillman 2003), anterior knee pain (Asplund and St Pierre 2004), and foot disorders e.g. paraesthesia and “hot foot”.
Historically the cleat was positioned so that the first metatarsal head lies directly over the pedal axle, however more recently this idea has changed to suggest that positioning the pedal axle beneath the third metatarsal head allows a more efficient transfer of power.
If the rider has a leg length discrepancy then the shoe-pedal interface can be adjusted by inserting a shim between the shoe and the cleat or by having a custom orthotic insole manufactured. Research suggests that anything greater than 6mm is considered significant and needs correcting (Silberman et al. 2005) although some athletes may not be able to tolerate a difference of 3mm (Baker 2000). If a rider has a leg length discrepancy then up to half the difference should be corrected. Any excessive malalignment of the lower extremity, such as forefoot varus or over pronation, can be corrected with the use of canted shims or wedges (Sanderson 1990).
The saddle
A common and under reported phenomenon amongst cyclists is numbness (Leibovitch and Mor 2005). This can present complexly, or be resolved by means of simply correcting the bike fit – evidence suggests looking at saddle height (too high and forwards), saddle shape (cut out and removing the long nose) and maintaining an upright position (Lowe et al 2004) beneficial for reducing pressure on the perineum.
ISM, Cobb, Rido and Specialized are all leaders in providing ergonomic and carefully thought out saddles, but products can also be limited by many fit systems which place clients into “neutral fits”. As a result the saddle may be the “perfect” height for pedalling, but not for other complaints which they may have.
The cranks
A great deal of research discusses the physiological effects of crank length, less studies investigate outcomes related to running shorter crank on cyclists with hip, knee and ankle pathologies. Reducing crank length in these clients, does, however, seem logical. Anecdotally I can report great success from switching those struggling with a closed hip angle to shorter cranks e.g. labral pathology, FAI, arthritic hips. Commercially you will struggle to obtain anything shorter than 165mm. Research does not appear to show shortening the cranks adversely affects power (Tomas, Ross & Martin 2010) and it may help with rapid acceleration in some situations (Macdermid and Edwards 2009).
***************************************
Bianca Broadbent MCSP ACPSEM, Physiotherapist at Physiokinetic, Spire & Fit Your Bike
www.spirehealthcare.com/littleaston/physiotherapy-at-spire-little-aston-hospital
With extra special thanks to:
Tim Pigott MCSP ACPSEM
Physiotherapist – Athlete Matters / Preston Physiotherapy & Sports Injuries Clinic
Academic lead – Clinical Biomechanics Salford University
Useful Links
Specialized BG http://www.specializedconceptstore.co.uk/body-geometry-fit/
Trek http://www.trekmk.com/bike-fitting/
Apex http://www.apexbikeperformance.com/
Torke https://torkecycling.com/
Bikefit.com http://bikefit.com/
Cyclefit http://cyclefit.co.uk/
Retul www.retul.com
Medicine of Cycling Research Library – http://www.medicineofcycling.com/research/
References
GREGOR, R. & WHEELER, JB. (1994) Biomechanical Factors Associated with Shoe/Pedal Interfaces. Sports Medicine, Volume 17, Issue 2, pg 117–131
FARREL, K. REISINGER, K. & TILMAN, M. (2003) Force and Repetition in Cycling: Possible Implications for Iliotibial Band Friction Syndrome. The Knee, Volume 10, Issue 1, pg 103-109
ASPLUND, C & ST. PIERRE, P. (2004) Knee Pain and Bicycling – Fitting Concepts for Clinicians. The Physician and Sports Medicine, Volume 32, Issue 4
LEIBOVITCH, I. & MOR, Y. (2005) The Vicious Cycling: Bicycling Related Urogenital Disorders. Eur Urol, Volume 47, Issue 3, Pg 277-286
LOWE, B. SCHRADER, S. & BREITENSTEIN, M. (2004) Effect of Bicycle Saddle Designs on the Pressure to the Perineum of the Bicyclist. American College of Sports Medidine, Pg 1055-1062
TOMAS, A. ROSS, E. & MARTIN, J. (2010) Fatigue During Maximal Sprint Cycling: Unique Role of Cumulative Contraction Cycles. Medicine and Science in Sports and Exercise, Volume 42, Issue 7, pg 1364-1369
MACDERMID, P. & EDWARDS, A. (2009) Influence of Crank Length on Cycle Ergonometry Performance of Well Trained Female Cross Country Mountain Bike Athletes. European Journal of Applied Physiology, Volume 108
AHONEN, J. (2008) Biomechanics of the foot in dance. Journal of Dance Medicine & Science 12:3 99-109
FOUSEKIS, J. TSEPSIS, K. & VAGENAS, G. (2010) Multivariate Isokinetic Strength Asymmetries of the Knee and Ankle in Professional Soccer Players. Sports Medicine and Physical Fitness. Volume 50, Issue 4, Pg 465-474
KRIVICKAS, L. (1997) Anatomical Factors Associated With Overuse Sports Injuries. Sports Medicine Volume 24, Issue 2, Pg 132-146
SILBERMAN, M. WEBNER, D, COLLINA, S. & SHIPLE, B. (2005) Road Bicycle Fit. Clinical Journal of Sports Medicine. Volume 15, Issue 4, Pg 271-276
BAKER, A. (2000) Medical problems in road cycling. In Gregor RJ, Conconi F, eds. Road Cycling, Oxford, UK. Blackwell Sciences Ltd, Pg 68-120
SANDERSON, D. (1990) The Biomechanics of Cycling Shoes. Cycling science. Pg 17-30.