
Further commentary:
Low back pain and sciatica: management of non-specific low back pain and sciatica
Draft clinical guideline February 2016
This commentary follows a previous blog post.
Late last Friday night I got around to dropping the pain VAS outcome figures from the trials of acupuncture versus sham into RevMan 5 – the software used for Cochrane Reviews. I was surprised to find that the high I2 value for the short-term outcome in the draft guideline did not drop substantially with the corrected data (incidentally there were errors in the data from both Brinkhaus and Leibing). Here is the corrected forest plot to replace Figure 667 [Appendix K, p 153].
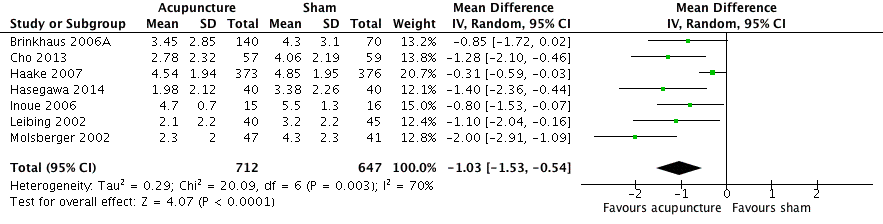
The total mean difference in pain now reaches clinical significance, and remember that is the difference over gentle needling, not an inactive placebo intervention. However, the heterogeneity remains unexpectedly high. The outlier now is Haake. This was a huge multicentre trial with some 300 different centres, where the participant clinicians did not meet for instruction on intervention procedures, as the 26 in Brinkhaus did. The primary outcome in Haake showed both real and sham acupuncture were twice as good as guideline based conventional care, so we might hypothesise that the sham was closer to real acupuncture than in Brinkhaus. Excluding Haake removes all heterogeneity.
So one large trial where we suspect substantial differences in the comparator (sham acupuncture) creates all the heterogeneity. But large trials are usually held out to be more statistically reliable, so there does remain some uncertainty in interpretation. I should point out that within RevMan the pain results for Haake are positive, so whether you think the sum of the smaller trials (n=610) or Haake (n=749) are more reliable, both demonstrate a biological effect of average acupuncture over gentle acupuncture.
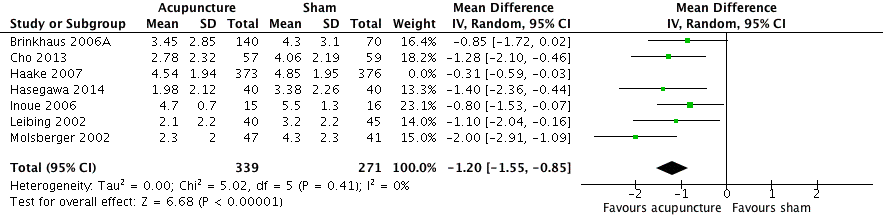
Moving to the long term analysis (pain VAS >4 month), there was a data entry error here too. Hard to spot, but glaring when noticed – the pain VAS outcome for Leibing was a negative value! How can a pain score be negative? The negative figure is clearly a change value, not an absolute value of pain at the relevant time point (this is the same data entry error made for the Brinkhaus data). Here is the corrected Figure 668 [Appendix K, p 153].

Statistically positive and no heterogeneity, this represents a clear long term biological effect of average acupuncture over gentle acupuncture, although the difference is not in the range that would be regarded as clinically significant by NICE, if indeed you can judge clinical significance in an explanatory (sham controlled) model. The heterogeneity result seems to be explained by a reduction in the mean difference between acupuncture and sham in the smaller trials, and no change in that of Haake, so in effect the smaller trial results got closer to the results of Haake. In terms of absolute pain scores, it seems that, on average, the patients in Haake continued to improve, whereas those in the smaller trials deteriorated slightly.
In summary, whilst there remains some uncertainty about interpretation of the clinical relevance of this data, it is clear that average acupuncture is superior to gentle acupuncture for low back pain in both the short and long term outcomes, and this data is clearly more convincing than the equivalent data for either the exercise or the manual therapies recommended in the draft NICE guideline for low back pain.
Declaration of interests
I am the salaried medical director of the British Medical Acupuncture Society (BMAS), a membership organisation and charity established to stimulate and promote the use and scientific understanding of acupuncture as part of the practice of medicine for the public benefit.
I am an associate editor for Acupuncture in Medicine.
I have a very modest private income from lecturing outside the UK, royalties from textbooks and a partnership teaching veterinary surgeons in Western veterinary acupuncture. I have no private income from clinical practice in acupuncture. My income is not directly affected by whether or not I recommend the intervention to patients or colleagues, or by whether or not it is recommended in national guidelines.
I have not chaired any NICE guideline development group with undeclared private income directly associated with the interventions under discussion. I have participated in a NICE GDG as an expert advisor discussing acupuncture.
I have used Western medical acupuncture in clinical practice following a chance observation as a medical officer in the Royal Air Force in 1989. My opinions are formed by data that spans the range of quality and reliability, much of which is in the public domain.
I have a logical mistrust of the motives of anyone who advertises an interest or hobby in being a ‘Skeptic’, as opposed to using appropriate scepticism within their primary profession, or indeed organisations that claim to promote generic ‘science’ as opposed to actually engaging in it.