
(Photo: Steve CC BY-NC-ND 2.0)
I have invited Dr Alex Donaldson (follow him on Twitter @AlexDonaldson13), of the Australian Centre for Research into Injury in Sport and its Prevention, to share a little more about their new paper published open access in Injury Prevention: “We have the programme, what next? Planning the implementation of an injury prevention programme“.
The Translating Research into Injury Prevention Practice (TRIPP) framework, developed by Caroline Finch a decade ago, built on van Mechelen and colleagues’ ‘sequence of prevention’ for sports injuries. TRIPP highlighted the fact that only research that can, and will, be adopted by sports participants, their coaches and sporting bodies will prevent sports injuries. Stage 5 of TRIPP (‘Describe intervention context to inform implementation strategies) introduced the (then) novel idea of focusing research attention on understanding how the outcomes of efficacy research (TRIPP Stage 4) could be translated into interventions (policies, programmes, environmental or technical modifications) that could be actually implemented in the real-world context. This included developing an understanding of the best way to target and market evidence-based interventions to sport bodies and their participants.
However, implementing injury prevention programmes in the real-world is challenging and there is precious little information available in the scientific literature about how to transition from having an evidence-based intervention to getting that intervention widely, properly and sustainably implemented. As a consequence, most research remains in the early stages of these models/frameworks (i.e. describing the extent of the problem and identify causes or mechanisms of injury) which limits the potential for injuries to be prevented.
In a soon to be completed study investigating the factors that influence the translation of evidence-based injury prevention interventions into practice in community sport, I (as the project manager) found myself in the situation where my colleagues and I had:
- Identified that lower limb injuries (LLI) were a significant problem in community Australian Football;
- Identified that research evidence suggested that a LLI prevention programme should include balance and control, eccentric hamstring, plyometric and strength exercises; and
- Developed a LLI prevention programme (now known as FootyFirst) including consensus from experts about the content of the programme.
What we then needed was an implementation plan for FootyFirst. The burning question was how can we ensure that the programme we had developed will be used and maintained for as long as it is needed by community-level Australian Football coaches and players?
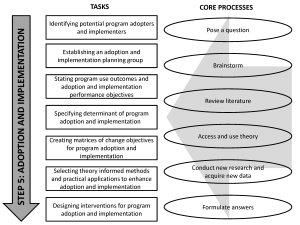
Luckily for me, I had recently attended a short training course facilitated by Guy Parcel (then Dean Emeritus of the University Texas School of Public Health (Austin) on Intervention Mapping (IM). IM is a framework for health promotion intervention development underpinned by the notion that the impact of a health promotion (or injury prevention) programme is a function of the programme (its efficacy) and its implementation (whether people actually use it properly for sustained periods of time). IM is a six-step tool for planning and developing health promotion programmes. Like other programme planning frameworks, it starts with needs assessment and ends in evaluation. However, unlike other frameworks, it includes a step (Step 5) specifically focused on planning programme adoption, implementation and sustainability. IM Step 5 comprises seven tasks that are operationalised through six core processes (see Figure 1) and can be used independent of the other IM steps.
The thing I found particularly useful about IM Step 5 was that it helped me to focus my attention on answering some key questions during the FootyFirst implementation planning process including:
- Who will decide to use FootyFirst and who will deliver it to the players?
- How can we involve the delivers (coaches) and participants (players) in developing the implementation plan for FootyFirst?
- What do community-AF coaches actually need to do to adopt and implement FootyFirst?
- What is likely to influence whether coaches adopt and implement FootyFirst?
- What needs to change for coaches to adopt and implement FootyFirst?
- What strategies could be used to help, support or encourage coaches to achieve the identified changes?
- Why do we think a particular implementation strategy is likely to work – what is the evidence or theoretical underpinnings for the selected strategy?
Programme effects have been shown to be up to three times higher when programmes are well implemented. If your target audience doesn’t know about your programme, use it properly and use it for a sustained period of time, it is unlikely your injury prevention programme will achieve the holy grail of ‘making a difference in the real-world’. For me, using IM Step 5 helped to ensure that our programme implementation planning process was:
- based on a partnership between health promotion, implementation science, and injury prevention researchers, and community sports administrators and coaches;
- informed by behaviour change theory, implementation science frameworks and published evidence about effective implementation strategies for safety programmes in community sport; and
- supplemented with in-depth knowledge of the implementation context and input from the programme end-users.
This in turn enabled us to develop an implementation plan specifically designed to bridge the gap between research (top-down) and community (bottom-up) driven programme implementation processes.
Our experience demonstrates the critical importance of researchers, practitioners and community end-users collaborating early in the implementation planning process underpinned by a mutual respect for the knowledge, skills and experience that these different groups bring to the implementation planning process.